TransformingtheWaitingExperienceforthe988Suicide&CrisisLifeline
A clinical, data-driven approach to improving emotional regulation and reducing chat abandonment during critical crisis wait times.
Role
Lead Product Designer & UX ResearcherSolo Project
Scope
- UX Research
- Usability Testing
- Interaction Design & Prototyping
- Stakeholder Presentation
Stakeholders
- Vibrant Emotional Health
- Substance Abuse and Mental Health Services Administration (SAMHSA)
Status
Approved by SAMHSA: In development with the dev team
Disclaimer
The views, opinions, and analysis expressed in this case study are the author's own and do not necessarily reflect the official views, opinions, or policies of the Substance Abuse and Mental Health Services Administration (SAMHSA), or the U.S. Department of Health and Human Services.
TL;DR
- —
Problem: The 988 Lifeline cut chat wait times dramatically, yet users in crisis were giving up sooner than ever, many only seconds away from connecting. A rotating carousel of tips wasn't enough to hold someone in acute distress through the wait.
- —
Approach: Following a Vibrant stakeholder recommendation against a wait timer (a standard consumer pattern that breaks down in a clinical context), I designed an evidence-based guided breathing exercise to add an active coping tool to the wait screen, grounded in crisis intervention research.
- —
Design goal: Reduce emotional escalation and chat abandonment during the wait by giving users something clinically grounded to do, while ensuring no one felt they might lose their place in line.
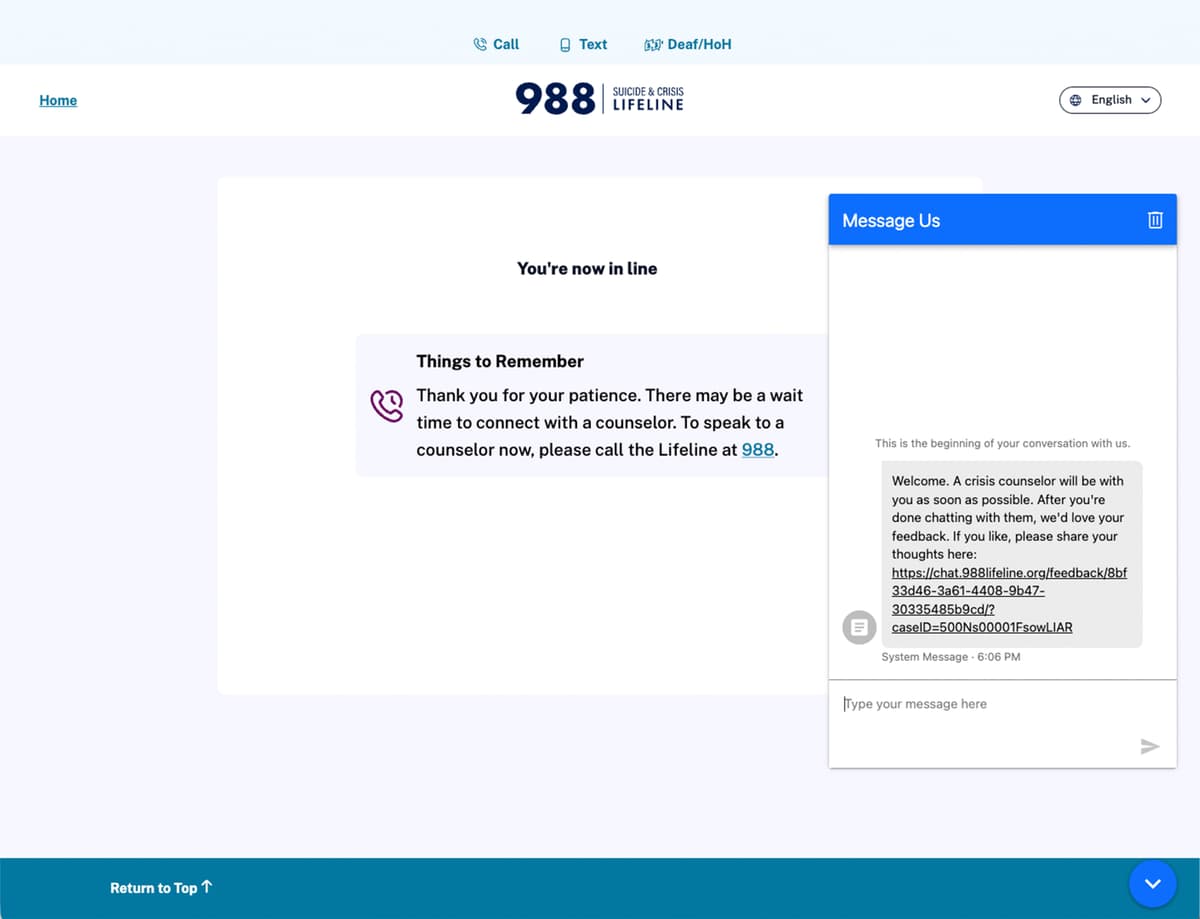
Before
MVP
The Paradox
Users in crisis were leaving faster even as actual wait times shrank. Between 2022 and 2025, the 988 Lifeline cut answered chat wait times from over 5 minutes to under 2 minutes, a genuine operational success. But abandonment data told a different story: the average user who gave up was doing so sooner than ever before.
Roughly 60,000 people reach out via 988 chat each month. Every one of them sits on this wait screen. At that scale, even a small improvement in how many people stay through the wait translates to thousands more people reaching a counselor.
~6 min
How long before users gave up, 2022
349 seconds of waiting before abandoning
2:21
How long before users gave up, 2025
Down to 141 seconds: giving up twice as fast
These figures measure how long users waited before abandoning, not how long it took to reach a counselor.
The Proposed Approach
The hypothesis: supplementing the existing wait screen with a low-effort, active coping tool would reduce premature abandonment by giving users something clinically grounded to do, keeping them engaged and emotionally regulated rather than fixated on the passage of time.
Several interventions were considered (static resource links, a mental health FAQ, background audio), but guided breathing was prioritized because it requires no reading, no content decisions, and delivers immediate physiological benefit regardless of literacy level or emotional state. Scientific research shows controlled box breathing is an effective technique for autonomic nervous system regulation: slowing the respiratory rate shifts the body from a fight-or-flight state toward a rest-and-digest state, naturally lowering heart rate.
Studies indicate box breathing can be more effective than mindfulness meditation at improving mood and reducing negative emotions, making it particularly well-suited to the acute distress state of someone waiting for a crisis counselor.
Industry Precedent
This pattern is validated across the crisis support landscape. Crisis Text Line surfaces resource links while connecting users to counselors. The Trevor Project offers a 1-minute guided breathing exercise before a help-seeker is ready to talk. Bringing a comparable capability to the 988 Lifeline aligns the product with established best practice, applied at significantly greater scale.
Testing the Solution
I led unmoderated usability testing via Qualtrics and Figma with 9 general population participants, measuring four dimensions: interest and willingness to engage, mobile discoverability, intuitiveness, and distraction potential. The sample was sized for qualitative signal and directional validation ahead of engineering investment (not statistical significance), consistent with standard practice at this stage of product development.
Key Outcomes (n=9 participants)
Interest & Willingness
Perceived Clinical Value
Intuitiveness
Discoverability
Ease of finding on mobile
Distraction level during exercise
“A good tactic to make you kind of chill until the person arrives.”
Mobile Discoverability Flow
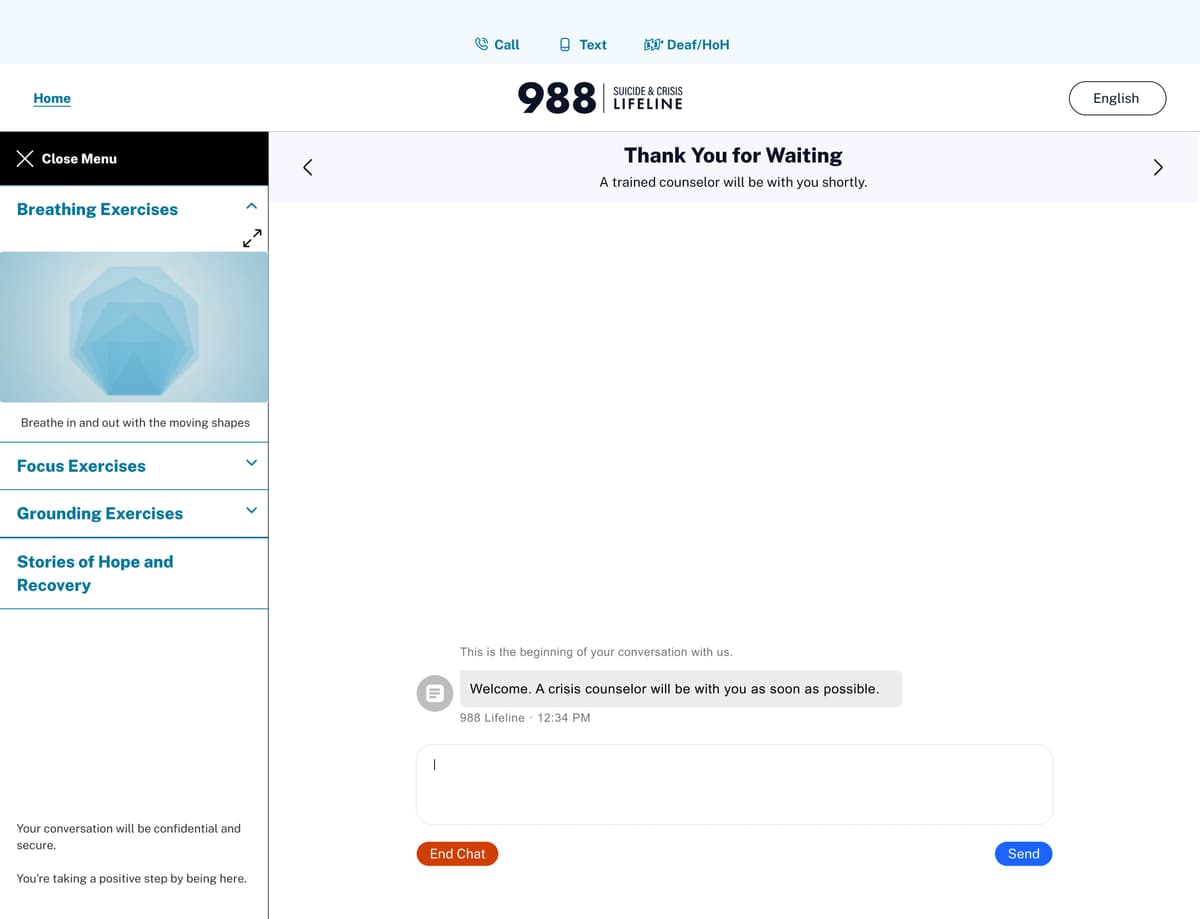
On mobile, the breathing exercise is accessed by minimizing the chat widget. To surface this affordance without cluttering the UI, a system message appears in the chat thread prompting users to tap the minimize button. 8 of 9 participants successfully accessed the exercise this way. The one participant who didn't noted the minimize button was “kind of hard to see,” feedback that informed the recommendation to increase the button's visual prominence.
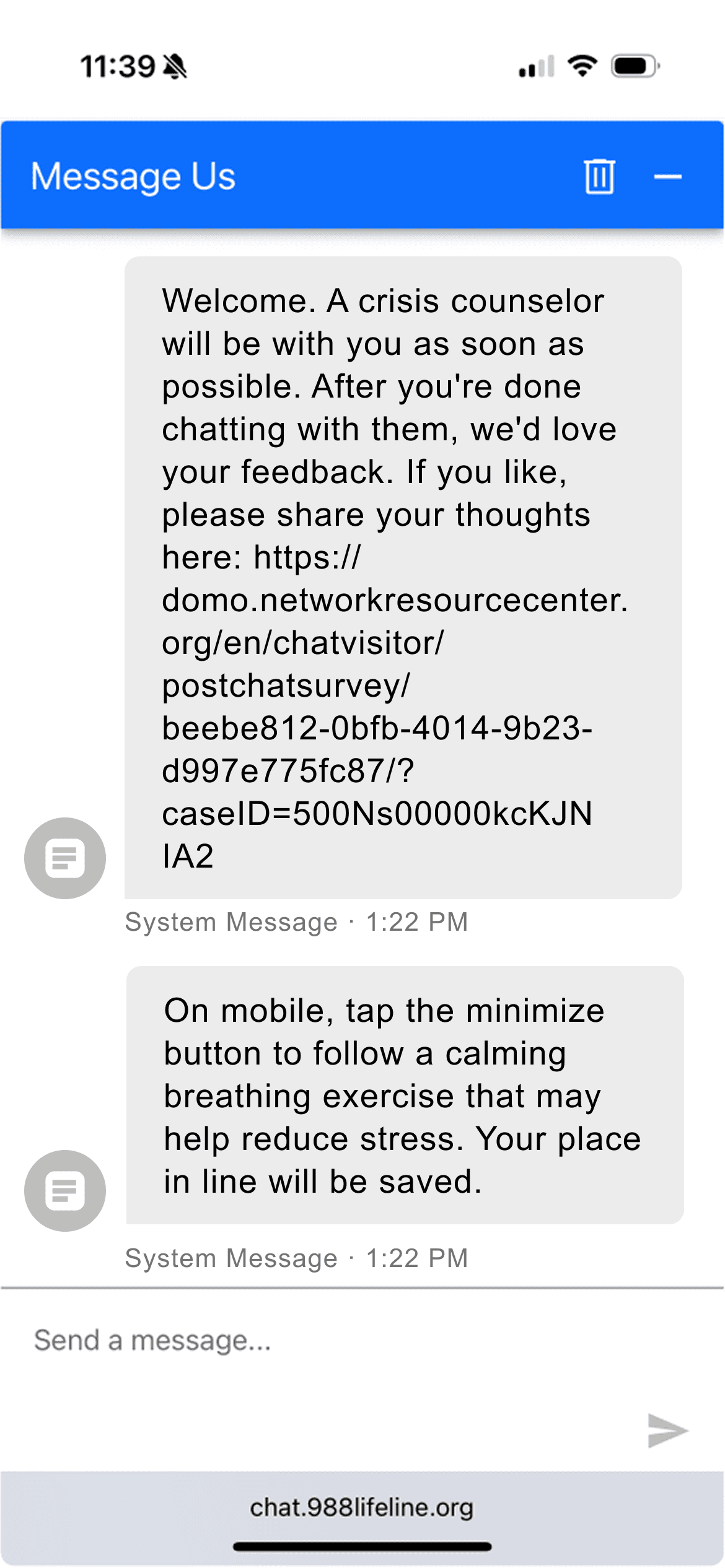
System message surfaces the minimize affordance

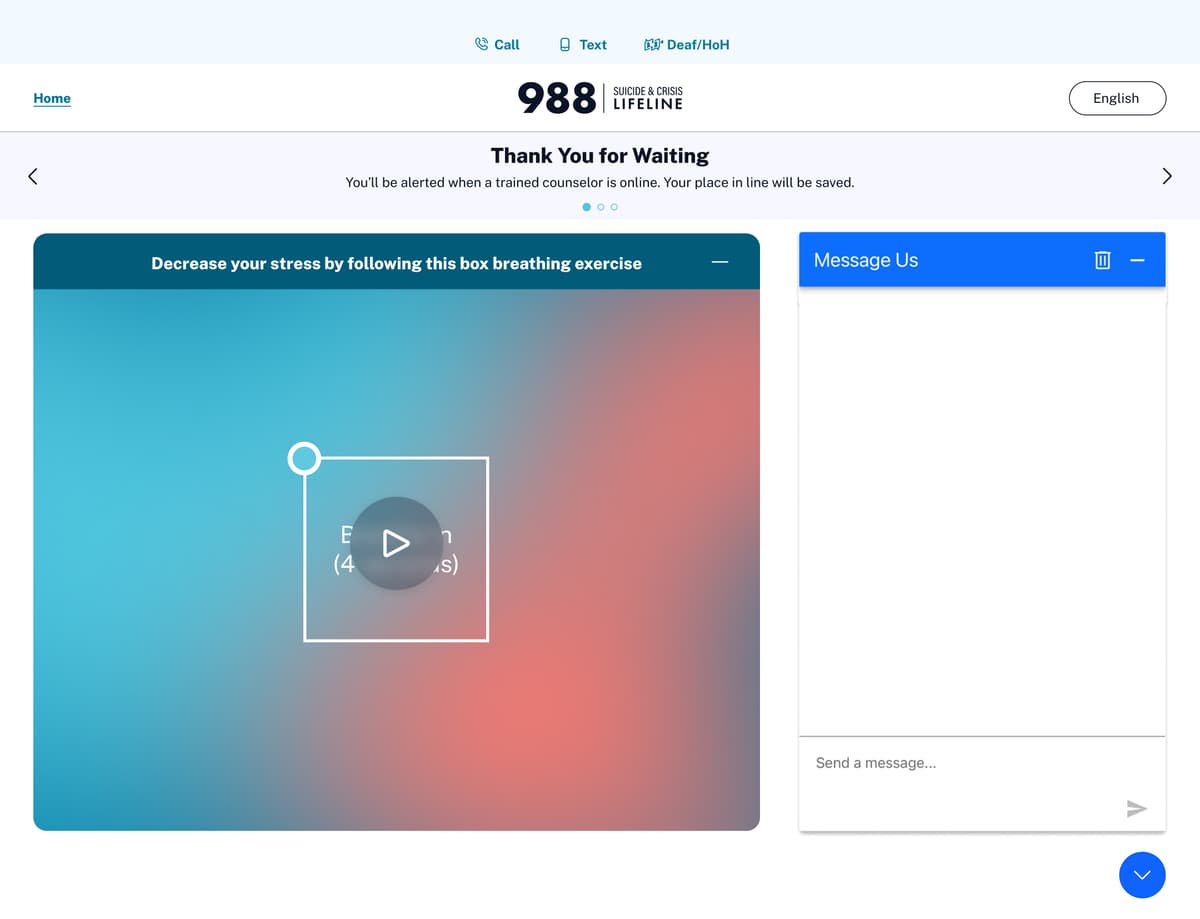
Exercise with queue reassurance banner
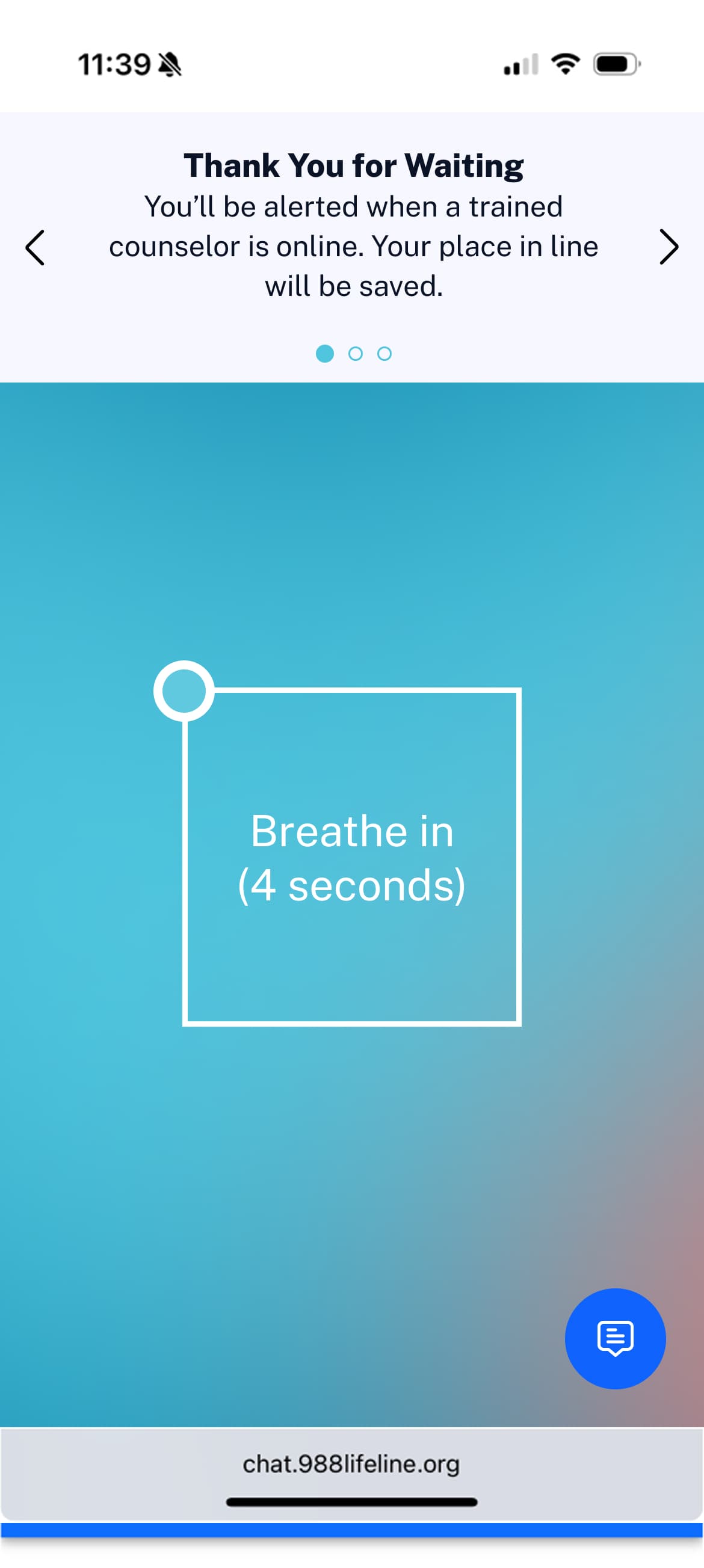
Box breathing: Breathe in (4 seconds)
The Distraction Divide
The study surfaced one primary tension: cognitive load during the exercise. Of 9 participants, 4 found it not distracting at all, 1 was neutral, and 4 found it slightly distracting. That near-even split warranted investigation rather than dismissal.
Qualitative follow-up identified two root causes. First, users feared engaging with the exercise might cost them their queue position. Second, the rotating automated message banner, which cycled through multiple notifications, competed with the breathing animation for attention, making it difficult to follow either.
Banner Copy: Before & After Survey
Shown to participants
“Thank you for waiting. A trained counselor will be with you shortly.”
Updated after survey
“Thank you for waiting. You'll be alerted when a trained counselor is online. Your place in line will be saved.”
The original copy gave no reassurance about queue position. The revised message directly addresses the primary friction surfaced in testing: users' fear of losing their place by engaging with the exercise.
A Constraint That Sharpened the Solution
During testing, multiple participants asked if the system could simply show an estimated time of arrival: “tell me he'll be there in like 5 minutes.” A visible ETA is standard UX practice in consumer support. A stakeholder team at Vibrant recommended against implementing one, and the reasoning was clinically sound.
Dynamic, Non-Linear Routing
The 988 backend dynamically prioritizes users based on active risk level. A queue position can change mid-wait. An inaccurate estimate (promising 3 minutes then taking 15 due to a routing change) would severely damage trust at exactly the moment when trust is most fragile.
Preventing Wait-Time Fixation
A visible countdown shifts cognitive focus entirely to monitoring the queue. This defeats the goal of emotional regulation and increases the likelihood of abandonment. The intent was to redirect attention constructively, not toward the passage of time.
Active Coping Over Passive Monitoring
A breathing exercise offers immediate clinical value regardless of how long the wait ends up being. A timer offers none. Given a choice between a therapeutic tool and a progress bar, the therapeutic tool serves the user's actual need.
MVP to North Star
The ideal future vision was a modular coping toolkit: an expandable side panel offering multiple evidence-based interventions: guided breathing, a focus exercise, and a grounding exercise, all accessible within the chat interface. This would have required engineering to rebuild the proprietary chat widget or source a third-party solution, introducing significant launch risk and delay.
I scoped a leaner MVP that worked entirely within the existing widget architecture — designing the breathing exercise to fit within currently available real estate (a side panel on desktop, a minimized fullscreen experience on mobile) preserved the core clinical value while dramatically reducing engineering level of effort and time-to-market.
MVP
Built within existing architecture. Faster to ship, lower engineering level of effort.
North Star
Modular coping panel with multiple interventions. Requires chat widget rebuild.
Shown: default state.
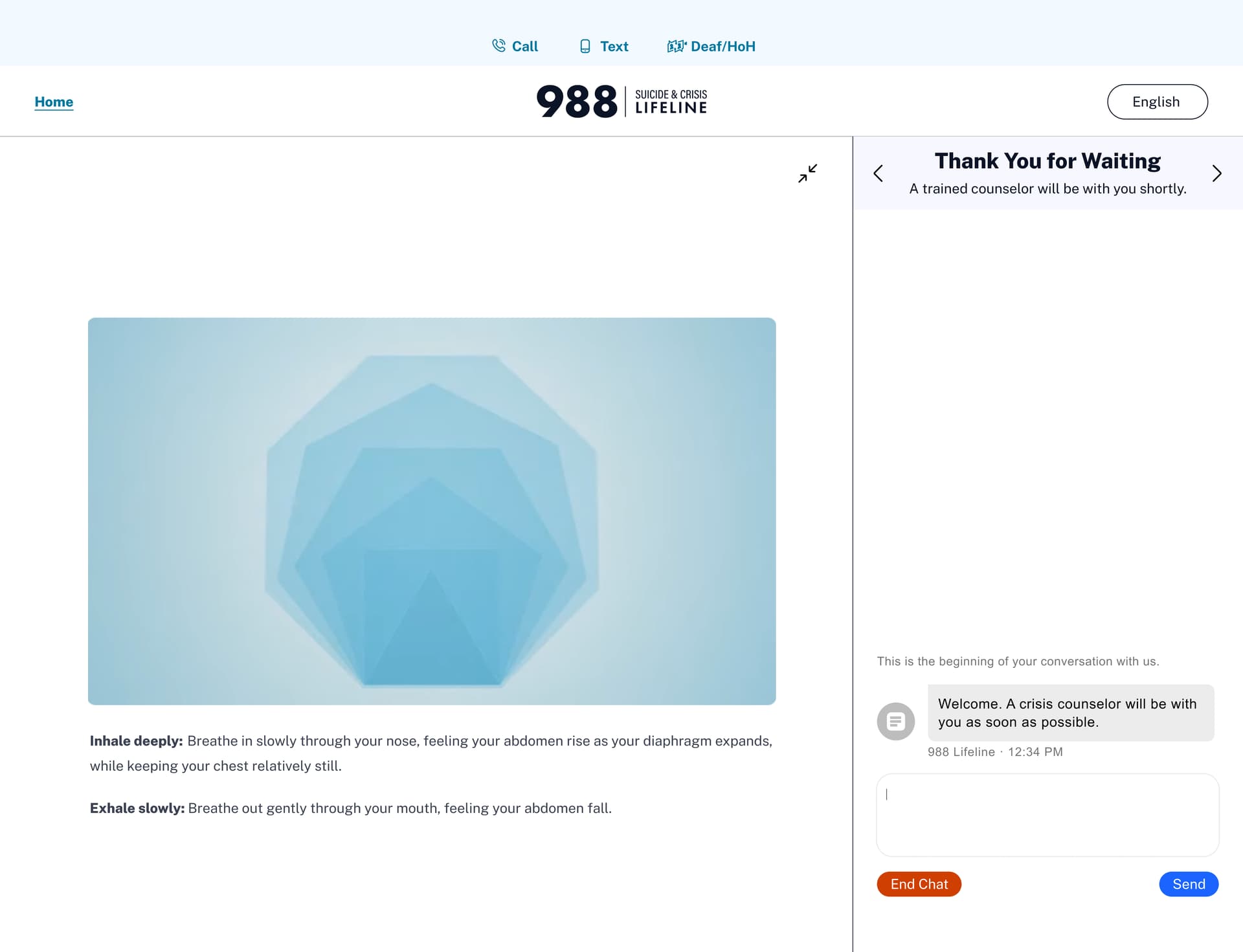
North Star: Breathing exercise maximized: full-screen animation with guided inhale/exhale instructions.
Interactive Prototype — Desktop
Interactive Prototype — Mobile
What's Next
SAMHSA has signed off on the design. The immediate next step is engineering handoff to build the validated prototype.
Stakeholder & SAMHSA Alignment
SAMHSA has reviewed and signed off on the validated prototype and UX findings. The design is approved and ready for engineering handoff.
Pre- & Post-Launch Analysis (GA)
Google Analytics instrumentation will enable a direct comparison of abandonment rates before and after launch, benchmarked against the 141-second baseline. Primary success metric: reduction in chat abandonment during the wait window.
Clinical Efficacy Measurement
The most meaningful success signal won't come from Google Analytics. It will come from counselors.
The plan is to prompt counselors to document self-reported visitor distress levels at the start of each chat session, creating a longitudinal dataset that connects wait experience quality directly to clinical intake outcomes. If users who engaged with the breathing exercise arrive in a measurably calmer state, that closes the loop between the UX intervention and the clinical goal. It also gives the counseling team a richer picture of who they're about to speak with.
Reflection
The hardest part of this project wasn't the design; it was validating a clinical intervention with consumer research methods. Usability testing tells you whether people can use something and whether they want to. It can't tell you whether it actually reduces distress. That gap is real, and the clinical efficacy measurement plan is my attempt to close it post-launch.
The 50/50 distraction split is the finding I'd investigate most in a follow-up study. My instinct is that the banner carousel is the root cause, not the breathing exercise itself, but I'd want a second round of testing with the carousel paused to isolate the variable before drawing conclusions.
Roughly 60,000 people reach out via 988 chat every month. Every one of them sits on this screen. That's the number that stayed with me through every design decision — and the reason the gap between a good-enough solution and a carefully tested one is worth closing.